Home
Subscription
May 2026 issue
April 2026 issue
March 2026 issue
February 2026 issue
January 2026 issue
BACK ISSUES
2025
2024
2023
2022
2021
2020
2019
2018
2017
2016
2015
2014
2013
2012
2011
2010
2009
2008
2007
2006
|
Each issue will include an editorial on a topic that is important for the profession of pharmacy, as well as a review of a new drug that includes a comparison of the new drug with previously marketed drugs that are most similar in activity, and a New Drug Comparison Rating (NDCR) for the new drug. Read on for this month's issue.
July 2018 Issue [Download PDF format]
In this issue:
• Editorial
• New Therapeutic Agents Marketed in the United States in 2017
|
EDITORIAL:
THE CORPORATE DESTRUCTION OF HEALTH CARE: Part 1
And Health Professionals are Letting It Happen!
I remember the time when physicians, pharmacists, other health professionals, and healthcare institutions such as hospitals had both the authority and responsibility for the decisions regarding the healthcare services, medications, and other products provided for patients, including costs. This "system" had significant shortcomings but it usually facilitated communication and positive relationships among patients and health professionals. HOWEVER, the pendulum has swung to the other extreme and become stuck there as drastic changes have occurred in the provision of health care. Health professionals still have extensive responsibility (and liability), but most now have severely limited authority for the decisions they are in the best position to make on behalf of their patients.
Most decisions pertaining to the provision of healthcare services and products and their costs are now made by corporation executives, economists, health insurance companies, and government agencies. One consequence is the sharp decline in the number of independent pharmacies, the number of individual and group medical practices owned by physicians, and the number of community hospitals that are not part of regional or national networks in which the authority of both local management and health professionals is substantially reduced. Another consequence is that many patients are denied the opportunity to personally select the physicians, pharmacists, and other health professionals they would prefer to use. But, most importantly, even with important advances in the knowledge, technology, and skills in the treatment and prevention of disease, the communication of health professionals with individual patients is less complete and less effective in assuring patient understanding of healthcare services, medications, and relevant devices/products. This situation results in the quality of health care falling far short of the potential that can be attained, and many dangerous, and even fatal, errors.
Prescription medications
The experiences and problems with respect to the use of prescription medications are typical of the challenges for the entire health care system. There can be no question that the physicians, pharmacists, and other healthcare professionals who are directly involved in the care of patients are in the best position to assess a patient's needs, and select, dispense, and monitor the use of her/his medications. However, most prescription "benefit" programs have restrictive formularies and time-wasting prior authorization policies that greatly limit a prescriber's authority. Pharmacies are required to accept the compensation and comply with the terms of prescription plans that have been developed unilaterally by pharmacy benefit managers (PBMs). Even when they are willing to do that, pharmacies July be excluded from PBM networks or placed at a severe competitive disadvantage when PBMs mandate and/or provide financial incentives for patients to use mail-order or other pharmacies they own.
Executives of chain pharmacies determine staffing levels that are often inadequate, and impose metrics with respect to the number and timing of prescriptions dispensed, immunizations provided, and anything else they can measure. The stressful work environment that results is a prescription for errors, which occur in such numbers and consequences that they are the most closely guarded secret of chain pharmacy management that consider them just a cost of doing business. If the public and our legislators knew the actual number and consequences of medication errors, they would be outraged! Large chain pharmacies such as Rite Aid, Walgreens, and Walmart pretend to have an interest in health care while at the same time they sell and promote tobacco products. This hypocrisy should be denounced and rejected, and consumers/patients should be urged to use pharmacies that do not sell these toxins.
Some chain pharmacies have had an important role in establishing and supporting many of the new schools of pharmacy. This situation is a major reason for which there are now more pharmacists than positions available in many parts of the country. Chain pharmacies now have even less incentive to provide acceptable working conditions for their pharmacists and technicians, and some have reduced the hours and/or salaries of their pharmacists because it is unlikely they will be able to find employment elsewhere. The stress, frustration, and criticism of their employers among chain pharmacists are at a level I have not previously heard, with the following serving as examples:
- "It is management by intimidation."
- "Techs are doing things they have no business doing, and I don't have time to check everything."
- "If I don't get out of here, I will wind up hating people."
- From a long-time pharmacist manager who is very concerned about losing his job because of not meeting metrics: "Metrics rule all! My supervisor thinks I spend too much time talking with patients. It is ok to share my information. I desperately need someone to speak with."
- From a pharmacist with a placement company: "Even some chain pharmacies that use our services do not wish to hire pharmacists who are leaving another chain in their area because they are so negative they have to 're-program' them."
- From a pharmacist who left her position in a chain pharmacy to accept a position in another practice setting for a salary that was much less than in her chain position: "I love my current job. And anytime I am having a bad day, I remind myself that I could still be at xxxxx."
Chain pharmacy executives mandate "more prescriptions faster metrics" that are highly stressful and error-prone, and a dangerous disservice for their customers. If they gave the same priority and effort to challenging and rejecting the unfair and inequitable policies and compensation of health insurance companies and PBMs, their interests, as well as those of their customers and employees, would be much better served. But corporate executives will not do that! PBMs are not needed! The profession of pharmacy has the abilities and opportunity to develop safer and more effective and efficient prescription benefit programs.
We are letting it happen
Pharmacists and other health professionals win occasional battles but we are losing the war, and an even greater corporate destruction of health care can result. But why is this situation continuing on a downward spiral? We have the knowledge, skills, and the opportunities for positive and personal relationships with our patients, communities, and legislators. Can it be that "We have met the enemy and he is us"? (first used on a poster to promote Earth Day and subsequently by Walt Kelly in a Pogo cartoon strip). Notwithstanding the admirable and extensive efforts of some of our colleagues, most health professionals and our associations have been too complacent and content with the status quo.
I started writing this editorial on Saturday evening and finished writing it on Sunday evening. On Sunday morning the following words on a piece of paper captured my attention:
"We are more apathetic than active, isolated than involved, callous than compassionate, obstinate than obedient, legalistic than loving."
I was not only reading these words but I was saying them out loud with others from a statement with the title "Confession of Sin – (Corporate)" used in the church service I was attending. Notwithstanding the different context in which the word "Corporate" was used, I can't ignore the timing in which I was using it in the title of this editorial.
I would like to think that I am promoting positive changes in pharmacy and health care through my advocacy and editorials. However, I must accept my share of the responsibility for the insufficient resistance to the evolving destruction of health care. I have not done enough!
We have not addressed the role of pharmaceutical and insurance companies, and the impact of high drug prices, and these will be discussed next month in Part 2 of this series.
Daniel A. Hussar
|
|
[To Top]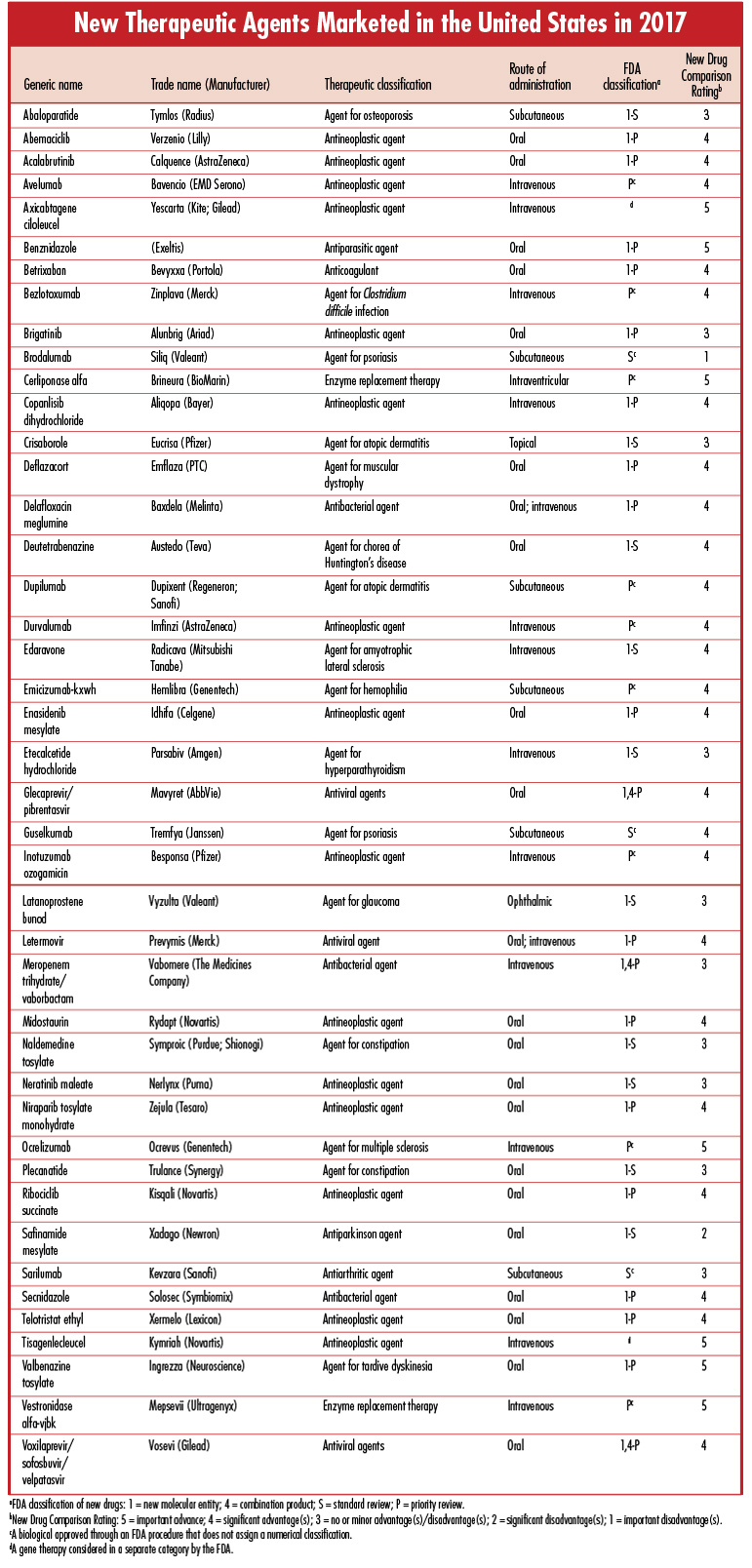
|
|